 Medically reviewed by
Medically reviewed by What is bipolar spectrum disorder?
There are several different definitions of BSD.1
There is also considerable debate over whether or not BSD even exists or has any diagnostic value.
According to Dr Elizabeth Brondolo and Dr Xavier Amador, the bipolar spectrum disorders are:
“a group of disorders all of which involve cycling moods. . . [BSDs] are also accompanied by a wide range of other symptoms that affect not just your mood but also your energy, your memory and thinking, and your connection with other people”.
Another expert who has done a lot of work in this area is Dr Jim Phelps. He points out that many people have symptoms: that are more than depression but less than bipolar.“
Dr Phelps has written a very well received book on bipolar ii and soft bipolar disorder called Why Am I Still Depressed? Recognizing and Managing the Ups and Downs of Bipolar II and Soft Bipolar Disorder.
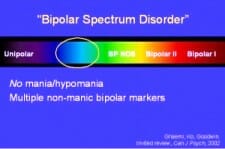
This describes bipolar spectrum disorder as the “Mood Spectrum”.
In the Mood Spectrum model depression and bipolar disorder are seen as the two opposite ends of a continuum, and people can be found all along the spectrum.
In other words, you can be at any point along the Mood Spectrum, and we can conceptualize different people’s symptom presentation as having different degrees of bipolar.
See concerns on “Underrecognized and Improperly Treated Bipolar Spectrum Illness” from the National Institute of Mental Health
The features of sub-threshold bipolar, (the mildest form of bipolar spectrum disorder, sometimes known as soft bipolar,) include:
A. At least one major depressive episode.
Reminder
Mood spectrum disorders involve emotional ups and downs, as well as cognitive problems.
B. No spontaneous hypomanic or manic episode.
AND
C. Either one of the following, plus at least two items from D, or both of the following plus one item from D:
- A family history of bipolar disorder in a first-degree relative.
- Antidepressant-induced mania or hypomania.
D. If no items from C are present, six of the following 9 are needed:
- Excessive emotionalism and/or excessive activity.
- More than 3 recurrent episodes of major depression.
- Brief major depressive episodes lasting less than 3 months.
- Atypical symptoms of depression such as increased sleep or appetite.
- Psychotic major depressive episode.
- Early age of onset of major depression (before 25).
- Postpartum depression.
- Antidepressant tolerance.
- Lack of response after trying more than 3 different antidepressants.
Bipolar Spectrum Disorder does exist, but is a problematic concept because of the danger of losing diagnostic rigor.
Responding to a diagnosis of BSD
What is the harm in broadening our understanding of mood disorders to accommodate the notion of a spectrum of bipolar?
In Manic-Depressive Illness: Bipolar Disorders and Recurrent Depression, 2nd Edition
It seems there are several dangers:
1. An on-going collapse of academic and clinical rigor.
2. Unnecessary prescription of strong medications such as the currently fashionable anti-psychotics.
3. Substantial self-diagnosis and self-medication, with the danger of treatment that is either unnecessary of inadequate.
4. Cultural trends that reward and romanticize mental illness in much the same way as we have erred in elevating a culture of victim-hood. Yes it is important to eliminate stigma, but do we want a society that embraces mental illness as a badge of honor?
However, there is also a substantial upside – more people getting the medication and/or therapy and other support they need instead of falling through the cracks.
A lot depends on what people DO with their diagnosis.
If folks are prepared to put the work into achieving stable moods through learning about appropriate medication, keeping a mood chart, developing a wellness plan and treatment contract, sleeping regular hours, and following the right program of diet and exercise, then success is almost inevitable.2
However, those who “fall in love” with their diagnosis of bipolar spectrum disorder and wallow in neurosis may have little to gain.
A spectrum of bipolar?

As this article explains, not all experts agree about the BSD: Subthreshold Bipolar Disorder – Not Ready for Prime Time
I am not a doctor and am unable to offer an informed opinion about the validity or usefulness of diagnosing up to 8% of the population of the US as having some form of bipolar.
At this stage I am a fence sitter. What I am sure of is that just as many folks with bipolar disorder still go undiagnosed, there are also many people – especially young people – who are being misdiagnosed as bipolar.
One 2010 research study from Rhode Island showed that people with borderline personality disorder are at particular risk of a misdiagnosis as bipolar.
There are also good reasons to believe that the recent 4,000% increase in diagnosing childhood bipolar is simply not credible, and must involve thousands of children with ADHD, Oppositional Defiant Disorder, Conduct Disorders, Major Depressive Disorder, or possibly no clinical condition at all, being seriously mislabeled.
Bottom line? There probably are a huge number of people for whom a diagnosis of a bipolar spectrum disorder would be helpful, especially if they educate themselves and incorporate lifestyle changes and therapy such as DBT or IPSRT into their recovery.
References:
1https://www.nami.org/Blogs/NAMI-Blog/March-2018/Understanding-the-Spectrum-of-Bipolar-Disorder
2https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5270687/