
Bipolar Type 2 Disorder: Symptoms, Diagnosis, and Treatment Guide
Bipolar II Disorder is a common but often misunderstood type of bipolar disorder. Learn its symptoms, diagnosis, and how it differs from Bipolar I.

ADHD and Depression: How They Overlap, Why They Co-Occur, and What Treatment Works
In my clinical practice, I often meet adults who describe their life as a “constant...

Rejection Sensitivity: What It Is, Why It Happens, and How to Cope
Have you ever had a friend take a few hours too long to text you...

Does Sertraline Cause Weight Gain? What Research and Patients Say
In my clinical practice, one of the most frequent and emotionally charged conversations I have...
Mental Health Conditions
Am I Bipolar?
Explore bipolar disorder basics including symptoms, types (I & II), causes, and more. Get clear, reliable info to better understand this condition and find support.
Bipolar Personality
Does bipolar disorder change your personality? Explore how bipolar affects traits, common misconceptions, and tips for managing identity alongside the condition.
Types of Bipolar
Understand the different types of bipolar disorder – Bipolar I, Bipolar II, cyclothymic, and others – with key differences in symptoms and severity explained.
Bipolar stories
Read inspiring bipolar stories from people living with the condition. Gain hope, insights, and practical tips from real-life journeys of managing bipolar.
Top Reads




Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
Featured Stories
- Bipolar II Disorder is a common but often misunderstood type of bipolar disorder. Learn its symptoms, diagnosis, and how it…
- In my clinical practice, I often meet adults who describe their life as a "constant uphill climb." One patient, "Elena,"…
- Have you ever had a friend take a few hours too long to text you back, only to find yourself…
- In my clinical practice, one of the most frequent and emotionally charged conversations I have with patients revolves around the…
 Sertraline is one of the most widely prescribed antidepressants in the world. When a patient sits in my office holding…
Sertraline is one of the most widely prescribed antidepressants in the world. When a patient sits in my office holding… When patients arrive at my clinic with a new prescription in hand, they often feel a mix of hope and…
When patients arrive at my clinic with a new prescription in hand, they often feel a mix of hope and…

Featured Mental Health Topics
Get Support
Read More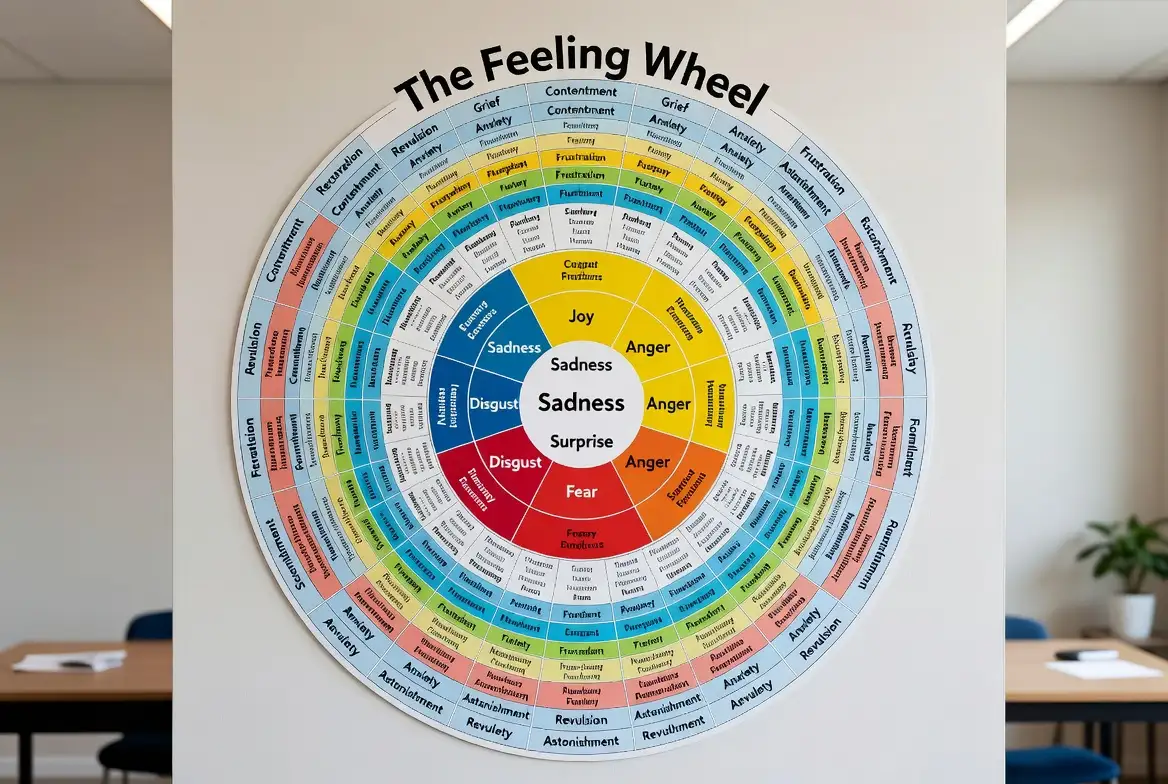
The Feeling Wheel: How to Identify, Understand & Express Emotions
At some point, we have all been asked, “How are you feeling?” and responded with a generic “fine,” “okay,” or...
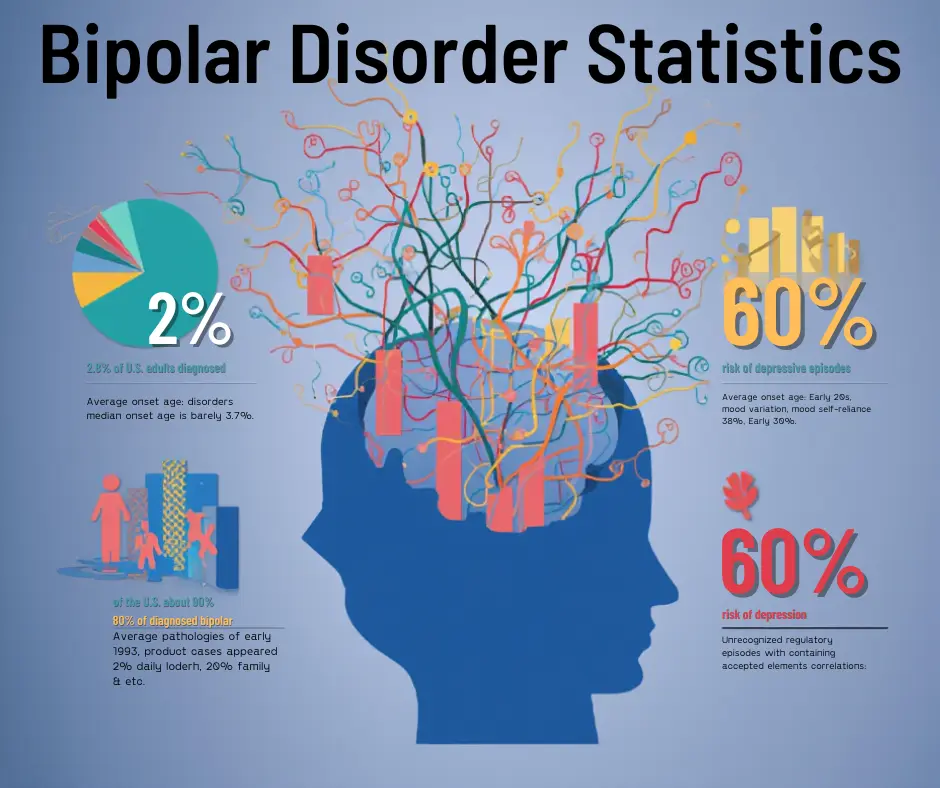
Bipolar Disorder Statistics, Facts & Treatment (2026 Guide)
Hey there. Are you looking for the truth behind the numbers? You are not alone in this search. Many people...

Emotional Intelligence: What It Is, Why It Matters, and How to Improve It
In the modern landscape of 2026, where technical skills are increasingly augmented by artificial intelligence, the human element has become...

Anxiety Medication: The Complete Guide to Options, Uses, and Alternatives
Anxiety is a natural human response—a biological alarm system designed to keep us safe from danger. However, for millions of...
Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential